by Hassaan Mazhar, Last updated: April 1, 2026

The Operational Reality No One Talks About
“A 15-minute video may take 3 hours.”
That’s how one hospital privacy officer described their current redaction workflow for Freedom of Information Act (FOIA) and legal requests.
Three hours of someone clicking frame-by-frame through CCTV or clinical video, trying not to miss a single face. Three hours of risk that one unblurred patient or visitor ends up in a disclosed video, creating a potential HIPAA incident. And that’s for one short clip.
Multiply that by dozens of requests a month — from FOIA, subpoenas, internal investigations, insurers, regulators — and you have a very real operational and compliance problem on your hands.
This is the daily grind that makes hospital privacy, risk, and security leaders uneasy: the growing volume of video-based requests, the inability to scale manual workflows, and the constant fear of missing a face in footage that clearly contains PHI.
This is exactly where on-premises video redaction for healthcare stops being a nice-to-have and becomes a necessary control.
The Problem: Manual Redaction Wasn’t Built for Today’s FOIA Reality
Let’s be blunt: traditional, editor-based workflows were built for creative teams, not for hospital privacy and compliance operations.
FOIA and legal requests increasingly demand video evidence: emergency department CCTV, hallway cameras, OR recordings, procedural videos, patient transport footage, even telemedicine sessions. These are all riddled with PHI and often show multiple patients, families, and staff in motion.
Yet the workflow in many hospitals still looks like this:
- Export video from VMS or clinical system
- Load into a desktop video editor
- Manually draw boxes over faces
- Constantly adjust as people move across frames
- Rewatch several times to make sure nothing was missed
This is slow, fragile, and difficult to defend in an audit. It makes it nearly impossible to respond to FOIA requests within statutory timelines and meet HIPAA’s minimum necessary and safeguarding requirements.
The result? Your team is stuck between two bad options:
- Rush and risk missing PHI in the footage
- Be thorough and risk missing FOIA or discovery deadlines
Neither is acceptable. That’s the core business pain: you can’t scale manual redaction, but you also can’t ignore the volume and sensitivity of today’s requests.
Where Manual Redaction Breaks Down in Healthcare
Manual redaction isn’t just slow. In a healthcare setting, it fails in predictable, high-risk ways.
1. Moving scenes with multiple patients
Think about ED waiting rooms, hallways outside imaging, or behavioral health units. People don’t stand still facing the camera. They walk, turn, sit, stand, and move across frames. Faces are partially visible, occluded, or appear only for a second.
In these environments, a manual editor is doing three cognitively heavy tasks at once:
- Detecting every face, often at different angles and lighting
- Tracking each face as it moves across the frame
- Applying a consistent blur or pixelation without gaps
It’s not realistic to expect perfection at scale. Fatigue sets in. Shortcuts happen. And the scenes with the highest risk (crowded EDs, behavioral health, pediatrics) are exactly the ones least suited to manual work.
2. Inconsistent standards across staff
Hospitals often rely on whoever is available — security, IT, legal, risk, or even clinical educators — to handle redaction in video editors. Each person interprets “PHI” and “face” slightly differently.
One person might blur every face in the frame. Another might only blur patients. A third might leave staff fully visible for context. Across dozens of requests and several years, this creates a patchwork of redaction decisions that is difficult to explain or defend.
In an OCR, discovery dispute, or regulator inquiry, this inconsistency can become a problem. You need a repeatable, rule-based process, not ad hoc operator judgment.
3. No clear audit trail
Desktop editors rarely provide the kind of audit logs compliance teams expect: who accessed which file, what changes were made, when, and based on which request.
When you produce redacted footage, you often can’t show:
- How many faces were detected and redacted
- Which frames were flagged as containing PHI
- Who approved the final version and when
From a compliance and eDiscovery standpoint, that’s a gap. In healthcare, the lack of documented process is a risk in itself.
Why Cloud-Only Tools Don’t Fit Hospital Data Governance
When teams realize manual redaction won’t scale, they often look at cloud-based tools as the next step. On the surface, it makes sense: upload a video, run automated redaction, download the result.
But in hospitals, this approach quickly runs into data governance walls.
PHI exposure and data residency
CCTV and clinical video are almost always PHI. Uploading this content to a multi-tenant cloud service, particularly one not designed for healthcare, creates exposure. Even with encryption, privacy and legal teams will ask:
- Where is this video stored, and for how long?
- Who at the vendor can access it?
- What happens if we need to purge it for legal or regulatory reasons?
If your organization has strict data residency, sovereign cloud, or on-prem mandates, many cloud-only tools are simply off the table.
BAA and vendor access concerns
Any service touching PHI must be covered by a Business Associate Agreement (BAA). Some video tools don’t offer BAAs at all. Others will sign one, but still retain technical access to your unredacted footage.
For privacy officers and CISOs, this is a red flag. They’d prefer a deployment model where:
- PHI stays within hospital-owned infrastructure
- Vendors have no direct access to content
- Auditability is in the hospital’s hands
Audit and eDiscovery requirements
FOIA, litigation, and regulatory investigations require clear chains of custody and defensible processes. With cloud-only tools, you’re reliant on the vendor’s logs, retention policies, and uptime.
For many health systems, that’s too much operational and legal risk to accept.
Why On-Premises Video Redaction for Healthcare Is the Logical Next Step
This is why more hospitals are turning to on-premises video redaction for healthcare as their primary model. It’s the only approach that simultaneously solves scale, automation, and data governance.
At its core, on-premises video redaction for healthcare means:
- Redaction software is deployed in your data center or private cloud
- All processing happens within your controlled environment
- PHI never leaves your network perimeter
This deployment model aligns with how hospitals already handle PACS, EHR, and VMS systems. It respects existing security architectures while introducing the automation you need to keep up with FOIA and legal demands.
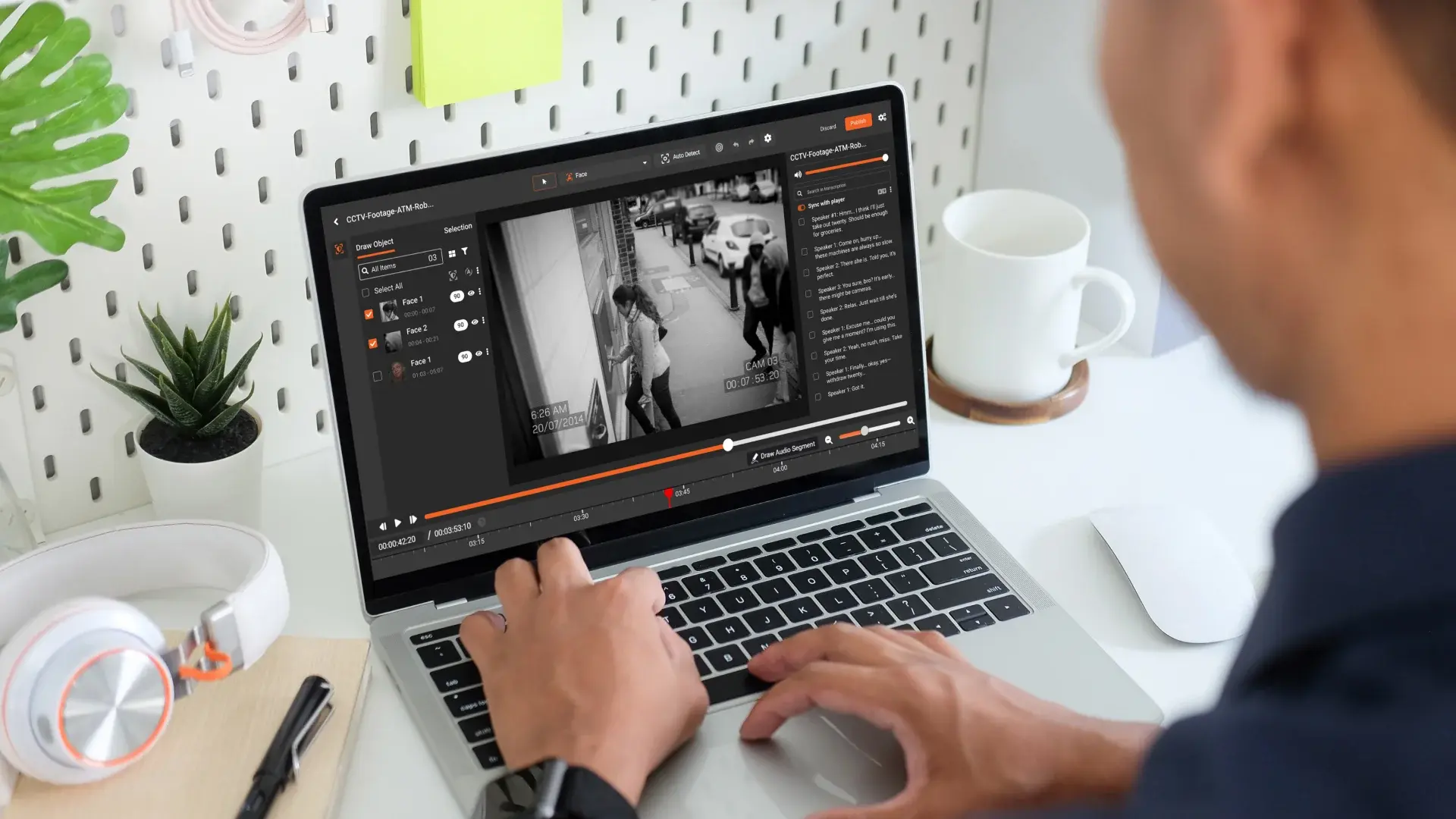
Automated face detection and tracking
Modern on-premises video redaction for healthcare platforms use AI to detect faces in each frame, track them as they move, and apply blur or pixelation automatically.
This matters for three reasons:
- Consistency: Every frame is treated using the same detection model.
- Speed: A 15-minute video can be processed in minutes, not hours.
- Defensibility: You can document how many faces were detected, what was redacted, and why.
Selective redaction: patients only, staff visible
In many FOIA and legal scenarios, you need to hide patients and visitors but keep staff visible for context. Manual workflows make that almost impossible at scale.
With a capable on-premises video redaction for healthcare solution, you can:
- Automatically detect all faces
- Quickly deselect staff faces that should remain visible
- Apply redaction only to patients and visitors
This “selective redaction” preserves evidentiary value and operational context while still protecting PHI.
Air-gapped deployment for maximum control
Some hospitals require complete isolation from the internet for sensitive systems. A mature on-prem video redaction for healthcare platform supports air-gapped deployments, allowing you to run the full stack without any external connectivity.
That means:
- No outbound data flows
- No vendor access to your content
- Full control over patching and upgrade windows
Key Capabilities to Look for in an On-Premises Video Redaction Solution
If you’re evaluating on-prem video redaction for healthcare, it’s not enough to tick the “on-prem” box. The details matter for both operations and compliance.
1. BAA support and healthcare orientation
First, confirm the vendor can sign a BAA and has experience with covered entities. You want a partner that understands HIPAA, FOIA, HITECH, and state privacy laws, not a generic media tool.
Ask about:
- Standard BAA terms and any gaps
- How they handle PHI if support access is ever required
- Reference customers in healthcare using on-prem deployments
2. Confidence tuning and quality control
AI face detection is powerful, but not infallible. You need the ability to tune detection confidence and review results.
Look for capabilities like:
- Configurable detection thresholds for faces
- Quick review interfaces to spot-check results
- Options to prioritize fewer misses (false negatives) over fewer false positives
For high-risk areas, you might set the system to over-redact and then manually unmask certain faces (like staff) as needed.
3. Redaction styles and granularity
Different workflows require different redaction types. Your on-prem video redaction for healthcare platform should support:
- Blur, pixelation, and solid fill for faces
- Ability to redact other identifiers (e.g., screens, name badges, medical record numbers)
- Audio redaction for spoken names or medical details
Granularity matters. In some cases, you may only need to obscure faces. In others, you might need to cover full bodies, screens, monitors, or whiteboards carrying PHI.
4. Robust audit logs
From a compliance standpoint, this is non-negotiable. You need:
- Per-user audit logs (who did what, when)
- Per-file history (versions, changes, approvals)
- Reporting you can export for auditors or legal teams
A mature on-prem video redaction for healthcare solution lets you show your work: which faces were detected, which were redacted, and who approved the final output.
5. Pilot-first evaluation model
Don’t commit to anything based solely on a demo. Demand a pilot where you can run your real-world footage through the system.
In this pilot, track:
- Time required per 15-minute clip using your current manual method
- Time required using automated, on-prem redaction (including review)
- Accuracy: proportion of faces correctly detected and redacted
This will give you hard numbers to take to leadership: how much time you can realistically save, and how much you reduce human error in PHI handling.
Introducing an On-Premises, HIPAA-Ready Redaction Platform
Once you’ve defined these requirements, you’ll find only a handful of platforms truly align with healthcare’s constraints. One of them is VIDIZMO REDACTOR.
VIDIZMO REDACTOR is designed for on-prem video redaction for healthcare environments that cannot move PHI to the public cloud. It offers:
- Automated face detection and tracking: AI-driven redaction that follows faces frame-by-frame, even in crowded, moving scenes.
- Selective redaction control: Redact patients and visitors while keeping staff visible, or apply broader redaction where required.
- On-prem and air-gapped deployment: All processing happens inside your network; PHI never flows to vendor infrastructure.
- HIPAA-ready architecture: BAA support, secure authentication, role-based access control, and detailed auditing.
- Flexible redaction styles: Blur, pixelation, solid fill, and support for other object and audio redaction as needed.
- Comprehensive audit logging: User actions, redaction runs, approvals, and exports are all tracked for compliance.
Hospitals have used VIDIZMO REDACTOR in pilot programs to benchmark time savings against manual workflows. Consistently, teams see a shift from “3 hours for a 15-minute clip” to around 30 minutes end-to-end, including review and approval.
That’s the practical impact of choosing the right on-premises video redaction for healthcare platform: you get automation and governance in the same stack.
Benefits Snapshot: From 3 Hours to 30 Minutes per Clip
To bring it all together, here’s what hospitals typically gain when they transition to automated, on-prem video redaction for healthcare:
- Dramatic reduction in manual effort: Pilot-validated reductions from ~3 hours to ~30 minutes per 15-minute clip, including human review.
- Scalable FOIA and legal response: Ability to handle higher volumes of video requests without growing headcount proportionally.
- Stronger HIPAA and privacy posture: Systematic, documented redaction that aligns with minimum necessary and safeguards requirements.
- Better data governance: PHI remains within your infrastructure; you maintain full control, with no uncontrolled vendor access.
- Defensible, auditable process: Clear logs and redaction histories you can present to auditors, regulators, or courts.
- Improved cross-team collaboration: Legal, privacy, security, and clinical operations working from a shared, reliable redaction process.
Ultimately, on-premises video redaction for healthcare is not just about technology. It’s about making sure your hospital can meet FOIA, legal, and insurance demands without burning out your staff or gambling with PHI exposure.
If your team is still saying, “A 15-minute video may take 3 hours,” it’s time to rethink the workflow.

About the Author
Jump to

How to Redact Body-Cam Footage for FOIA Requests

Best Redaction Software for Law Enforcement (2026 Guide)

No Comments Yet
Let us know what you think