by Ali Rind, Last updated: May 11, 2026

Clinical trial redaction is the process of removing protected health information (PHI), commercially confidential information (CCI), and other sensitive data from clinical trial documents before they are shared with regulators, partners, or the public.
Sponsors, contract research organizations, and clinical operations teams handle thousands of pages per study, including clinical study reports (CSRs), protocols, informed consent forms, case report forms, and adverse event narratives. Each document carries patient identifiers, investigator details, and proprietary methodology that must be removed before disclosure.
This guide is written for clinical operations leaders, regulatory affairs teams, and IT directors designing or upgrading a clinical trial redaction workflow. It covers the current regulatory drivers, the data categories that need redaction, where manual processes fail, and what to look for in modern redaction software.
Key Takeaways
- Clinical trial redaction addresses two distinct categories: PHI under HIPAA Safe Harbor and CCI under EMA Policy 0070 and Health Canada PRCI.
- A single Phase III submission can generate tens of thousands of pages of redaction-eligible content, with each redaction defensible and traceable to a justification.
- Manual redaction averages 4 to 8 minutes per page. AI-assisted workflows with human review reduce this to under 1 minute per page in production.
- Modern trials produce non-document evidence too: investigator interviews on video, telehealth visits, lab images with embedded metadata. A document-only tool leaves compliance gaps.
- The defensible audit trail (who redacted what, when, under which exemption) is what regulators inspect, not the redacted file alone.
What Is Clinical Trial Redaction?
Clinical trial redaction is the systematic removal of identifiable patient data and commercially sensitive information from clinical trial documents before disclosure. It sits at the intersection of patient privacy law (HIPAA in the US, GDPR in the EU, PIPEDA in Canada) and pharmaceutical transparency mandates (EMA Policy 0070, Health Canada PRCI, and emerging FDA initiatives).
The discipline has two distinct objectives. The first is protecting patient identity. The second is protecting the sponsor's intellectual property. These goals frequently conflict. Regulators want maximum disclosure for scientific transparency. Sponsors need to protect synthesis routes, formulation details, and statistical methodologies that took years to develop. The redactor's job is to satisfy both.
In practice, redaction teams handle four document streams per study: the CSR and its appendices, the protocol and statistical analysis plan, individual patient narratives and CRFs, and supporting items like investigator brochures, manufacturing documents, and pharmacovigilance reports. PHI rules apply across all of them. CCI rules apply mainly to the protocol, the CSR body, and manufacturing sections.
For PHI redaction in clinical research more broadly, including HIPAA workflows for research teams, see our guide on how to automate PHI redaction in medical records.
Why Clinical Trial Redaction Matters More in 2026
Three forces have pushed clinical trial redaction from a niche regulatory task into an operational priority.
The first is regulatory expansion. After a five-year suspension, the EMA relaunched Policy 0070 in September 2023, with Step 2 going live in May 2025. The latest external guidance (Version 1.5) was published in May 2025 and broadened the scope of in-scope applications. Health Canada's Public Release of Clinical Information regulation has been in force since March 2019 and has expanded steadily through device and biologic submissions.
The second is volume. Modern programs generate substantially more content than legacy ones. Decentralized trials produce telehealth recordings. Investigator training is delivered on video. Patient-reported outcomes arrive from mobile apps with embedded device metadata. The artifact mix has shifted from paper CRFs to digital evidence.
The third is enforcement. EMA's Clinical Data Publication portal does not just accept your redaction package. It audits a sample. Inconsistent redactions, missing justification codes, and patient identifiers leaking through into supposedly redacted files all trigger re-review, which adds weeks to the disclosure timeline.
How EMA Policy 0070 and Health Canada PRCI Drive Redaction Work
The two transparency regulations driving most clinical trial redaction work are similar in spirit and different in detail. Both require sponsors to publish clinical data once a regulatory decision is made, and both allow redaction of personal data and CCI.
EMA Policy 0070 organizes redactions into two anonymization approaches: full anonymization (removing all direct and indirect identifiers using statistical risk methods) or pseudonymization plus redaction. Every CCI redaction must carry a justification mapped to a structured code, typically pointing to a category such as manufacturing know-how or commercially sensitive market data.
Health Canada PRCI follows similar logic with different exemption categories. Sponsors submit a redaction proposal that Health Canada reviews before publication. Over-redaction of clinical safety data is the most common reason for rejection.
Both regulators publish the final documents permanently. There is no take-back if a patient identifier leaks through. The redaction has to be right the first time.
What Data Must Be Redacted in Clinical Trial Documents
The data needing redaction in clinical trial documents falls into three categories: PHI, CCI, and indirect identifiers.
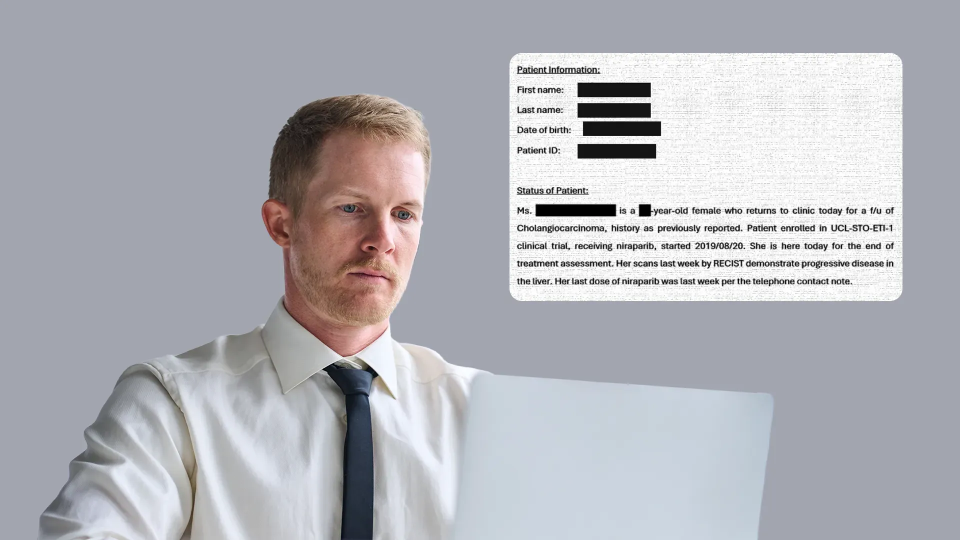
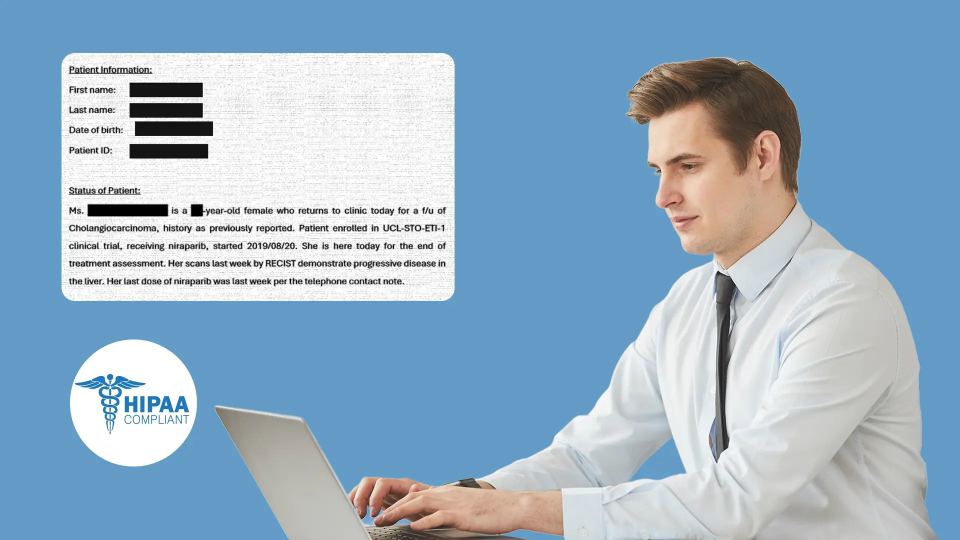
PHI under HIPAA Safe Harbor (45 CFR 164.514) covers 18 specific identifier types. In clinical trial documents these typically appear as:
- Patient names, initials, and study IDs that map back to identity
- Dates more granular than year (date of birth, visit dates, dates of procedures)
- Geographic detail smaller than state (city, ZIP code, address)
- Phone numbers, fax numbers, email addresses, IP addresses
- Medical record numbers, health plan beneficiary numbers, account numbers
- Device serial numbers, biometric identifiers
- Full-face photographic images and comparable images
- Any other unique identifying number, characteristic, or code
CCI varies by sponsor but commonly includes manufacturing know-how, novel formulation details, proprietary statistical methods, third-party data not covered by data-sharing agreements, and competitive market intelligence.
Indirect identifiers are the trickiest category. A 47-year-old male patient with a rare oncology subtype enrolled at a single site in Iceland is identifiable through combinations, even with name and address removed. The redaction team has to decide which combinations cross the re-identification threshold, applying statistical disclosure control where needed.
Why Manual Redaction Fails at Clinical Trial Scale
Manual redaction works fine for small documents. It collapses at clinical trial scale, and the failures tend to cluster around three issues.
The first is consistency. When eight reviewers redact across a 10,000-page CSR, redaction decisions diverge. Patient ID 042 is redacted in volume 3 but accidentally left in volume 7 because reviewers had different mental models of the policy.
The second is throughput. A skilled redactor handles 60 to 100 pages per day on dense clinical content, with QA adding another 30 to 50 percent of that effort. A 10,000-page submission therefore needs 100 to 200 person-days. Compressing this into four to six weeks usually means staffing temporary teams, which feeds back into the consistency problem.
The third is scope. Manual document tools cannot handle the non-document evidence that modern trials generate. Investigator training videos, telehealth recordings, scanned source documents from paper-based sites, and DICOM medical images with embedded patient metadata all sit outside the document-only workflow. Teams either skip these (creating compliance risk) or process them in separate tools (creating chain-of-custody gaps). For a deeper look at why general-purpose document tools fall short here, see why Adobe fails at clinical trial document redaction.
How to Build an Automated Clinical Trial Redaction Workflow
An automated clinical trial redaction workflow has five stages: ingestion, AI detection, policy mapping, human review, and audit-ready output. Skipping any stage breaks the workflow.
Ingestion
handles the format diversity of modern trials: PDF, Word, Excel, PowerPoint, scanned image PDFs requiring OCR, DICOM medical imaging, audio recordings, and video. A platform that only handles PDF will not cover the trial.
AI detection
finds candidate redactions using named entity recognition for PHI patterns, regex with context for country-specific identifiers, and visual AI for faces and identifying objects in images and video. Confidence thresholds matter here. Set them too low and reviewers drown in false positives; too high and PHI leaks through.
Policy mapping
is where many automated systems fall short. Detecting "1985-04-12" as a date is easy. Deciding whether to redact it as a date of birth, partial-redact it to keep the year per HIPAA Safe Harbor, or leave it as a study milestone date requires policy logic that has to be configurable per study and per regulator.
Human review
is non-negotiable. The defensible audit trail requires a human to approve or reject every redaction decision and document the justification. The platform's job is to make that review fast, not to eliminate it.
Audit-ready output
produces three artifacts: the redacted document, the unredacted master with redaction overlay so reviewers can verify, and the audit log mapping every redaction to a reviewer, timestamp, and justification code.
How AI Detects PHI and CCI in Trial Documents
AI detection of PHI and CCI combines three techniques: pattern matching with regex, named entity recognition (NER) using NLP models, and contextual classification using large language models for ambiguous cases.
Pattern matching catches structured identifiers like Social Security Numbers, dates, and email addresses. NER models identify free-text identifiers that do not follow rigid patterns, such as patient names, investigator names, hospital names, and disease names. Contextual classification handles the gray zones, deciding whether "Dr. Smith reviewed the case" refers to an investigator to redact or a published reference to keep.
The highest-leverage tuning is the confidence threshold. The default 80 percent setting is rarely right for clinical trials. Phase III submissions usually run at 60 to 70 percent (more candidates flagged, more reviewer effort, better recall on edge cases). Internal QC documents can run higher.
What to Look for in Clinical Trial Redaction Software
Selecting clinical trial redaction software comes down to seven criteria. Use this as an evaluation framework, not a feature checklist.

The criterion most sponsors underweight is deployment flexibility. Pre-approval CSRs often have legitimate reasons to stay inside the corporate network. A SaaS-only tool may not pass IT security review for those documents.
Compliance Standards for Clinical Trial Redaction
Clinical trial redaction touches multiple compliance frameworks. The most important ones for 2026:
- HIPAA Privacy Rule (45 CFR 164.514): Safe Harbor de-identification of 18 identifier types, or Expert Determination by a qualified statistician.
- EMA Policy 0070: Justification codes per CCI redaction; PPD anonymization per Version 1.5 guidance.
- Health Canada PRCI: Redaction proposal with structured exemption rationale, reviewed before publication.
- GDPR (Article 17, Article 89): Right to erasure, research data minimization.
- ICH E6(R3) Good Clinical Practice: Finalized January 2025 and now in force across major regions (FDA published guidance September 2025, EMA effective July 2025). The R3 revision strengthens records management, data integrity, and audit trail requirements that apply to redaction decisions.
The audit trail requirement deserves special attention. ICH E6(R3) requires that every change to study records be traceable. A redaction is a change. The audit trail produced by the redaction platform becomes part of the study's essential record, and inspectors can ask for it years after the trial closes.
How VIDIZMO Redactor Supports Clinical Trial Workflows
The format coverage and audit trail problems described earlier in this guide are exactly what VIDIZMO Redactor is built to solve. A Phase III submission rarely consists of documents alone. Investigator interviews, telehealth visit recordings, training videos, and scanned source documents from non-US sites all need redaction, and processing them in separate tools creates the chain-of-custody gaps that inspectors flag. Redactor handles documents, scanned images, audio, and video in one platform, with OCR for handwritten and scanned source materials and a single audit trail covering every format.
ICH E6(R3) requires every change to study records to be traceable, and a redaction is a change. The chain-of-custody log captures who redacted what, when, and under which justification, and exports as part of the study's essential record. Inspectors who ask for redaction rationale years after trial closure get a complete answer, not a reconstruction.
Pre-approval CSRs often cannot leave the corporate network, which rules out SaaS-only tools. Redactor offers SaaS, government cloud, on-premises, and air-gapped deployment, so sponsors can run pre-approval submissions on-premises and post-approval transparency packages in the cloud, on the same platform and under the same audit framework. Start a free Redactor trial to test it against your actual document mix.
About the Author

Jump to
NER in Healthcare: Redacting Clinical Entities from Unstructured Text
How to Make Your Healthcare Data Workflows HIPAA Compliant

No Comments Yet
Let us know what you think